
The intervertebral disc has long been acclaimed to be one of the main causes of back and sciatic type pain. Society has deemed them to be the bringer of a lot of misery and as a result they have gained a notorious reputation. But what are these much feared and maligned pieces of anatomy and are some of the claims about them true?
What are intervertebral discs?
The intervertebral discs are fibrocartilaginous joints that sit between vertebral bodies (vertebra) in the spine.
There are 23 of them in total; six in the neck, twelve in the mid back and five in the lower back. Each vertebrae has a corresponding number based on the vertebra between which it sits. For example C6/7 means between the 6th and 7th cervical vertebra. The letters change according to the location of the problem. For example C for cervical (neck), T for thoracic (mid back), L for lumbar (low back) and S for sacrum although there is only one that involves the sacrum (L5/S1)
The discs have a number of functions:
- Allow slight movement of each vertebrae and in turn the spine
- Add stability to the spine- like a ligament
- Shock absorption for the spine
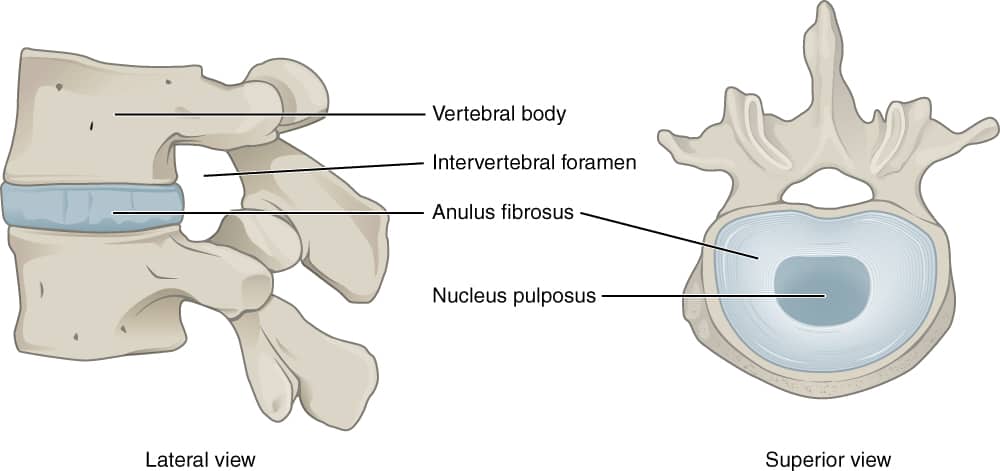
They have various design features that help them do these jobs effectively. They are composed of two rings. The outer ring is known as the annulus fibrosus which is composed of multiple layers of tough fibrocartilage. The inner layer is known as the nucleus pulposus. This is very much different in that it contains loose fibres in a gel like substance. The tough layer adds stability and strength whilst the gel-like layer allows for pressure to be distributed evenly.
The discs are held in place by what is known as the vertebral endplate. This fixes the annulus layer to vertebra and is very, very strong.
MYTH NUMBER 1- DISCS SLIP
This is a phrase that I hear lots and I am sure a phrase many of you have come across in your lifetimes. But hear me now, 100% discs do not and can not slip. They are fixed so well by the end plate that they simply can’t.
However that is not to say discs cannot get injured. We know they can get injured and terms that better reflect what has happened include herniation, prolapse or bulge. Now these things are real phenomena. What happens with these (and they all mean the same thing to a larger or smaller level) is that pressure is exerted from inside the gel like substance. This pushes against the tough outer layer, sometimes pushing through and sometimes just causing the outer layer to deform.
The theory goes this increased size of the disc then causes put pressure on other structures including the nerves leading to pain. Interestingly however this does not always happen
MYTH NUMBER TWO- DISC BULGES ALWAYS CAUSE PAIN
Interestingly a number of studies have looked at disc bulges in pain free people. The graphs below shows the amount of these people who had disc bulges. The numbers are surprisingly high even in younger people and are higher for necks than the lumbar spine.
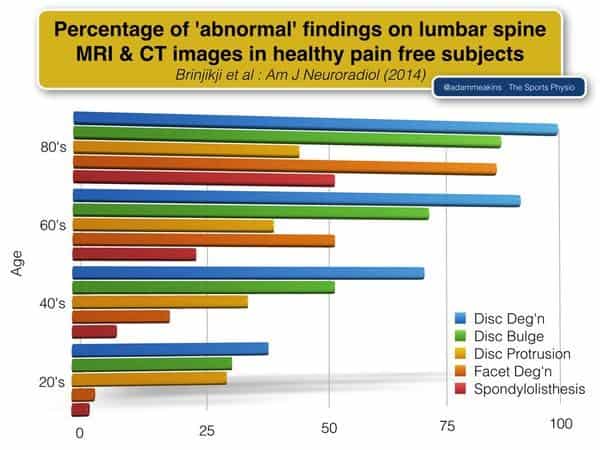
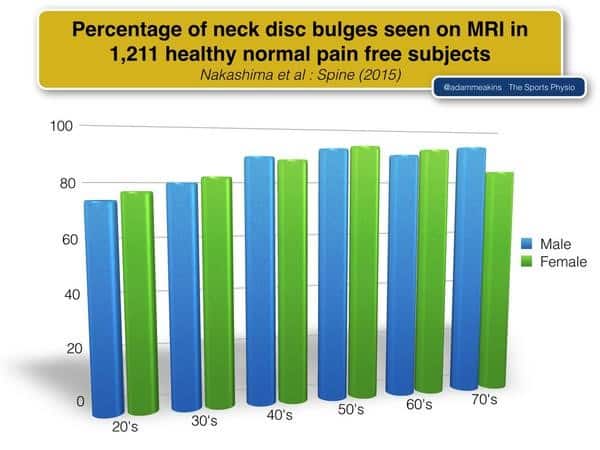
This tells us that the disc bulge cannot always be assumed to be the cause of a persons pain even if we find them on MRI. You are not your scan. The disc bulge may be a contributing factor but equally it may not. Pain is much more complex than you think.
When we do organise MRI, unless we have previous imaging we do not know if any bulges found are new or if it is one that pre-existed the injury. Thus it does not tell us the whole story and is sometimes why a disc bulge is sometimes referred to as an incidental finding.
That said if there is large disc bulge that is causing significant reduction in the space for the spinal cord and/or nerves, then it can be assumed that the disc bulge is having a bigger role in a persons pain. This is particularly if it matches the clinical picture with nerve like symptoms in the corresponding area of the leg. Surgical treatment may be an option however needn’t be the only or first option.
The only time it should definitely be the first option is if you have what is known as cauda equina. This is a more serious condition where an unprotected area of the spinal cord very low down in the back has pressure on it (e.g. from a disc). This is a medical emergency and so if you do get back and leg pain with any of the symptoms below, then please, please, please get yourself down to A and E pronto
Cauda Equina Symptoms (VERY IMPORTANT)
- Severe pain down both legs
- Altered sensation around your genitalia / back passage
- Faecal or urinary incontinence
- Reduced flow when weeing
- Feeling like you are not emptying your bladder
- Erectile Dysfunction
- Significant leg weakness
However Cauda Equina is very rare (lifetime incidence of just 1 peron per 100,000). Remember also many of these symptoms can also be explained by other medical problems and only 0.04% of the population presenting to A and E have cauda equina. Therefore, if you do have these symptoms don’t panic but DO get checked out and get it ruled out as it can have devastating consequences.
As I said before Cauda Equina is the only occasion where surgery should be the first option. This is because you can and many people do recover from disc injuries
MYTH NUMBER THREE- DISCS NEVER GET BETTER
Disc bulges do get better. Many studies have looked in to this and disc bulges do resolve. In many cases MRIs taken at a later date show them to be smaller or gone. Interestingly the bigger the bulge the quicker and the larger the degree of healing. So if you have been told you have a massive disc bulge it may be a good thing. One study has shown that up to 66% of discs resolve spontaneously. Many of these within a few months as shown in the picture below. However sometimes it can take up to a year so patience with these problems is king. In truth there is very little we can do to speed up human healing despite what some might say.

Equally interesting is that in these studies the degree of resorption of the disc is often unrelated to the degree of symptom recovery. By this some I mean that the disc in some people fully absorbs but there pain remains. Whilst in other people the bulge on a later scan looks exactly the same but there symptoms have much improved. The reasons for this is complex but recovery does not need to mean the disc bulge has receeded. The disc bulge is not the be all and end all. Many other factors play a part in the pain experience.
MYTH NUMBER FOUR- BENDING AND LIFTING IS DANGEROUS FOR DISCS
This old adage comes from a number of studies in the 80s which found that bending and lifting increases the intervertebral disc pressure. The findings were then extrapolated to mean that bending and lifting were the cause of disc problems and therefore frequently of back problems.
This information then snowballed through society. Initially this was likely through medical professionals including physios but then later gathered momentum from the likes of manual handling training, personal training and the media. Bending and lifting became a feared thing.
BUT
There are many flaws with what has happened:
Firstly the initial studies firstly looked at cadavers. I.e dead bodies with no active stabilisers such as the muscles working. Our bodies are likely to work much differently under these conditions. This has been realised ore recently as our technology has developed to allow us measure disc pressure in real time in alive humans. The evidence coming out from some of these studies suggest extension movements cause more pressure in the areas discs are likely to bulge.
Secondly these early studies did not demonstrate that increased pressure was necessarily a bad thing. This was just an assumption. These were purely biomechanical studies.
Is load or pressure a bad thing? Think about it. What do we do when we strengthen muscles? We put load though them, they adapt and they then become stronger. Similarly we know increased weight bearing activity early in life reduces osteoporosis risk. Runners have healthier cartilage and less arthritis than non-runners.
Increased forces in these examples appear to be a good thing. They have caused positive changes to keep tissues healthy. Could the same happen in discs? Suggestive of this is that one study has found improved hydration of discs in runners and in longer distance runners improved disc height. Pressure and load may therefore be a good thing.
MYTH NUMBER FIVE: DISCS ARE FRAGILE
Discs can tolerate huge loads. They are not the vulnerable things society as a whole has always assumed they are. For example one study looked at the compressive and tensile strength of discs. They found it takes 740lbs of pressure to compress a disc 1mm in 28 year olds and 460 lbs in 70 year olds.
These are big, big loads. Bear in mind also that this study used discs cut out from cadavers. They had no bony support and no muscular contractions. The forces in real life are therefore likely to be much, much higher.
As with all tissues, discs have a capacity to tolerate load. If we place load on them that exceeds their capacity then injury can occur. However as explained this capacity is remarkably yet sensibly high. The great news is that can be increased through exposure to load i.e. movement and exercise!!
Shear forces that arise as a result of side bending or twisting particularly in combination with bending may cause more load than bending alone. This is reflected in how many injuries from these types of movements. However, these shear forces are also just as likely to injure ligaments as they are discs and so pain after these may represent ligament sprains / tears rather than disc issues. Discs are no more fragile than ligaments and should definitely not be feared.
SUMMARY
Discs serve a number of functions in the spine. There are two layers: a tough inner and a gel like inner. Discs are very strong tissues and require large forces to injure. Discs do not slip. When discs injure they tend to bulge. This is not an issue most of the time and disc bulges exist in people without pain. A large proportion of disc bulges repair themselves and even in the absence of repair people can recover anyway. This is due to the deep and many complexities of pain.
Bending / lifting is not as dangerous as often thought and actually twisting is the larger problem of the two. That said discs can tolerate a lot of load. The more we load our backs the stronger they become. Movement and exercise therefore should not be feared. It should be the cornerstone of treatment for both recovery and future prevention.
If you have or have had a back problem and think it could be disc related or if you want to see what you can do get back on track then get in contact.
Here at Weymouth Physiotherapy we treat you as a person and not just a condition to get you back doing the things you want or need to do in as few sessions as possible.