The following is one of a series of articles looking to dispel myths about diagnosis of pain problems. I would recommend reading my general article on structural dysfunctions first as it provides good background reading. If you have ever been told your pain is due to a curve in your spine, your flat feet, your posture, or a leg length discrepancy then read on. If you suspect that these problems or other problems may be causing you pain also read on. Even if you are just curious then it would be great to have you on board.
Spinal Alignment
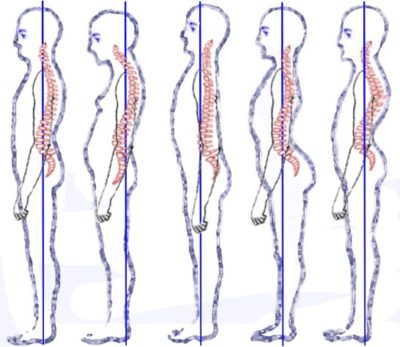
First up, spinal alignment. From the side view our spine has a series of curves that is often described as an S-shape. We have what is called a lordosis (backward c shaped shaped) in the cervical spine (neck), a kyphosis (c-shaped) in the thoracic spine (mid back) and another lordosis in the lumbar spine (lower back). From a front on view the majority of peoples spine are straight up and down. If there is a curve to one side we call it a scoliosis.
The other issue here is that without complex surgery these aren’t really correctable. Sure we can correct them in some people, by a small amount for some of the time however the spine is a solid structure and no amount of force through manipulation nor muscle strengthening or lengthening can change it significantly on a long term basis. An interesting thing to note is even in those corrected by surgery a surprisingly high number still struggle with pain afterwards. There is clearly more at work here than alignment alone. Yes these spinal differences may add load to particular areas however it is not the full picture.
Leg Length Discrepancies
Supposedly easy to measure and can be used to explain pain in many areas from the lower limb, to the spine and even in some cases compensations that lead to pain in the shoulder girdle for example. The truth however is that 70% of people have a leg length discrepancy. How much of leg discrepancy matters is up for debate. People have argued anywhere from 3mm-60mm is clinically significant. My argument is that if 70% of us have a discrepancy then why don’t 70% of us have problems.
The measurement of leg length discrepancy has also been shown to be unreliable, different between assessors and even within the same assessor at a different time interval. I suspect there is a high amount of bias at play, those that look for discrepancies find them. We see what we want to see, we find what we want to find.
If you have survived to adulthood without needing corrective surgery and have not had major trauma (fractures) it is likely your leg discrepancy is longstanding. Your body will have adapted to this. This could be by a number of ways for example pelvis tilting or rotating, hips rotating, knees bending. By trying to correct for leg length discrepancies it will put all this out of kilter. Leave it alone and concentrate your attentions elsewhere as a solution to your pain.
Lower limb alignment
The lower limb can be considered one kinetic chain. By this I mean they are to a degree all interrelated particularly when it comes to biomechanics. Starting at the hip the main thing that we look out for here is the rotation. The hip can be rolled inwards (anteversion) or backwards (retroversion). The width of the pelvis also has a part to play and may change the angle with which the thighbone (femur) travels to the knee. Something we call the Q angle, which is wider in females than males. At the knee itself there may be valgus (knock kneed), varus (the opposite of valgus), fixed flexion (unable to get fully straight) and hyperextension. The kneecap may also sit high (alta) or sit laterally (often due to hip and ankle anomalies). Further down the leg the shin bone may be internally or externally rotated and your ankle joint may be valgus or varus, all affecting the way in which your foot points. Finally, you may have flat feet which will have an impact on all the other biomechanical adaptations I have listed.
What relevance do all these have? Sometimes lots and sometimes little. Being honest I take each case on individually. I do think lower limb biomechanics are more relevant than alignment issues listed already, particularly at the knee which is in the middle of the chain. Each of the listed factors can cause stress on specific structures of the body and there is no doubt that this can contribute to pain. However, on the flip side there is often many people with the similar biomechanics who manage perfectly well with no pain. There is obviously something missing here, we can consider the biomechanics the kindling but we still need a spark to cause the fire. Finding this spark is the hallmark of a good therapist.
I believe that clinicians rely on their ability to spot these problems too much and then use them as their treatment focus. Sadly, often we can never fully solve these issues (without surgery and/or orthotics), they are often anatomical in nature and no amount of strengthening / stretching will correct them. Often rather than try to change the biomechanics we need to accept that they are there and instead focus on how we can compensate for them by modifying load and strengthening areas to offload the joint / structure.
Summary
In summary we are all different beings, we have all developed differently and all have different body shapes accordingly. Too much emphasis is placed on what is normal. Our definitions of normal are too narrow. Yes, alignment issues can cause certain areas/structures to be overloaded however there is often little we can do about it. I prefer to focus on building capacity to tolerate load, rather than trying to change the alignment issue at fault. Get your alignment issues nullified by booking an appointment today.